Cover Story
ALZHEIMER’S: NEW LEARNINGS, RISING HOPE
SINCE ITS DISCOVERY 118 YEARS AGO, THE BRAIN DISEASE HAS STYMIED RESEARCHERS. BUT THAT HAS BEGUN TO CHANGE, AND FOR THE FIRST TIME, WAYS TO PREVENT, SLOW AND EVEN TREAT THE DISEASE ARE EMERGING
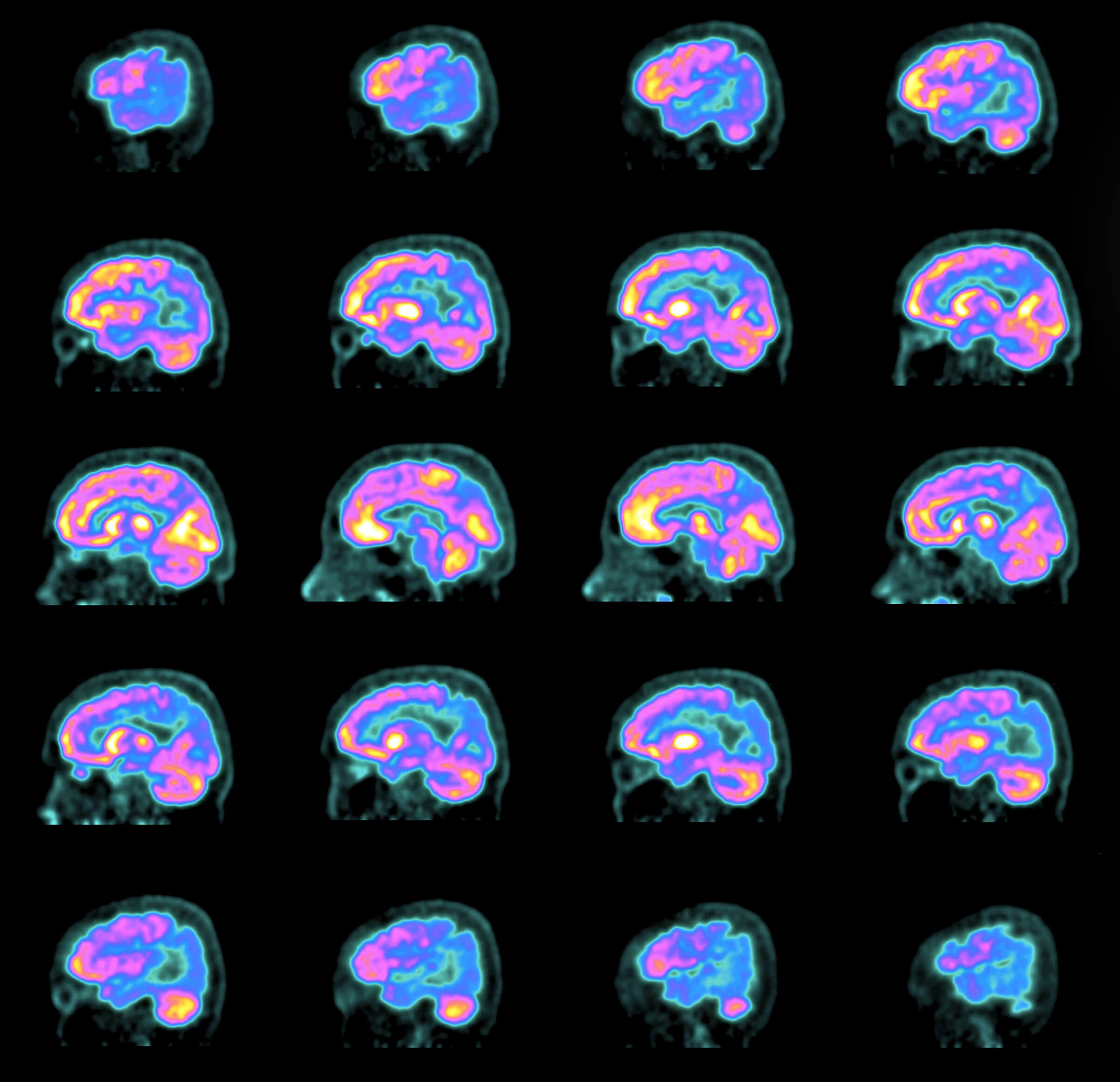
PET scans of the brain of a 58-year-old woman diagnosed two years previously with Alzheimer’s disease
Leonard Chayrez called his partner in a panic.
“I couldn’t remember how to use the credit card machine at the gas station, so I drove to three,” says Chayrez, a retired floral designer in Phoenix. “I kept forgetting things.”
That was in 2018. One year later, Chayrez, 58, was diagnosed with mild cognitive impairment, and shortly thereafter, Alzheimer’s disease. Since June 2023, he has received twice-monthly infusions of lecanemab (Leqembi), the headline-grabbing medication approved last year by the Food and Drug Administration that removes Alzheimer’s hallmark plaques from the brain and slows down memory loss. “I think I’ll have more days of happiness,” Chayrez says.
6.7 million
the number of older Americans who are living with Alzheimer’s disease
It is a measure of how bleak the outlook for patients was that lecanemab garnered so much attention—and hope. It isn’t a miracle drug. It doesn’t stop, reverse or cure this mind-robbing disorder; on average, it can slow mental decline by a mere five months over an 18-month treatment period, the research says. It comes with dangers of its own, including the risk of brain swelling and bleeding. Studies are ongoing. But despite all these drawbacks, it represents a huge breakthrough, a foundation on which the medical community can finally begin to build.
Neurologist and Alzheimer’s researcher Randall Bateman, M.D., puts it this way: “This is the beginning of the ability to treat, and change the course of, Alzheimer’s disease.
THE FIRST LITTLE VICTORY
Only patients with early-stage symptomatic Alzheimer’s disease and confirmed high levels of amyloid proteins in the brain are candidates for lecanemab. In a 2023 community-based Mayo Clinic study, only 8 to 17 percent of those were eligible based on the trial criteria. And its costs—an estimated $6,636 annually, even with Medicare coverage—are prohibitive for many.
Yet after more than 40 years of studies, tens of billions in research funding, at least 146 failed drugs and plenty of public controversy and private despair among scientists, the approval of lecanemab marks a major turning point in the fight against Alzheimer’s. It’s the first “disease-modifying” drug for Alzheimer’s to receive traditional FDA approval and win standard Medicare coverage. Most significantly, lecanemab is one in a handful of recent advances expected to—at last—transform how the medical community diagnoses, treats and eventually prevents one of America’s most-feared diseases.
“I’ve been doing this for 45 years,” says geriatrician and neuroscientist Howard Fillit, M.D., cofounder and chief science officer of the Alzheimer’s Drug Discovery Foundation. “This really is a watershed time.”
Over the next five years, scientists anticipate more breakthroughs: convenient blood tests to diagnose Alzheimer’s in your doctor’s office; a variety of drugs that can attack the disease on many different fronts; and customized, research-proven lifestyle strategies that will likely become standards of care. Within 10 years, scientists say, Alzheimer’s may be handled in your doctor’s office the way heart disease and diabetes are now—diagnosed via blood tests and treated with a combination of drugs and lifestyle strategies. The dream of patients, doctors, researchers and society: Instead of a terminal disease, Alzheimer’s could become treatable, preventable—and even reversible.

Leonard Chayrez (left, with his partner, Mark Garrity) has been taking the anti-Alzheimer’s drug lecanemab since June 2023. “I think I’ll have more days of happiness,” he says.
NO TIME TO WASTE
It’s a race against time. By 2030, 8.5 million older Americans are projected to have Alzheimer’s. A half-million of us will develop it this year.
Once it begins, there’s no way to halt it. As brain cells die, connections between them wither and the brain itself shrinks, memory worsens, thinking skills decline and navigating everyday life becomes less and less possible. At least a third of people with early-stage Alzheimer’s slip into a more severe stage in about three years, putting lecanemab and possibly other early-stage treatments out of reach. Because heredity plays a role, many of us with a family history of Alzheimer’s have long looked to the future with dread.
“For the first time, we can bend the curve of cognitive decline. ... But it’s not good enough. We need a home run.”
—REISA SPERLING, M.D.,
director of the Center for Alzheimer Research and Treatment at Brigham and Women’s Hospital in Boston
Rochelle Long, 67, of Shaker Heights, Ohio, cares for her 86-year-old mother with advanced Alzheimer’s while working full-time. Her father, grandmother, four aunts and an uncle all had the disorder. So far, she’s OK, but optimism comes hard. “Drug companies have spent how many billions of dollars through the years, and this is where we are?” Long says. “It’s disheartening.”
Even the most optimistic experts agree that lecanemab itself won’t turn the tide—but it could become part of an arsenal that can. “For the first time, we can bend the curve of cognitive decline,” says Harvard Medical School neurologist Reisa Sperling, M.D., director of the Center for Alzheimer Research and Treatment at Brigham and Women’s Hospital in Boston. Sperling is heading a new study looking at lecanemab to prevent Alzheimer’s in people at risk. “As a neurologist who takes care of patients and someone whose father and grandfather died of the disease, I think an extra five to six months of relative stability and independence is worth it,” she says. “But it’s not good enough. We need a home run.”
And at last, the medical community may be getting its turn at bat.
WHY IS THIS SO DIFFICULT?
Across the pharmaceutical industry, up to 90 percent of all experimental medicines that reach clinical trials don’t make it to market, either because they don’t work or they have bad side effects. Alzheimer’s drug research has an even higher failure rate. From 2004 to mid-2021, 98 experimental Alzheimer’s drugs failed in later-stage human studies. More were abandoned in labs or early human trials. Not a single new drug for Alzheimer’s was approved by the FDA for nearly 18 years. Among the research community, “people were despondent; it was like a clinical depression across the field,” Bateman says.
“The reason we’ve been so focused on plaques for so long is that they really stand out as soon as you look at the brain. ... You see these giant, ugly balls all over the brain.”
—KYLE TRAVAGLINI
scientist at the Allen Institute for Brain Science in Seattle
One major obstacle has been the historical difficulty of diagnosing Alzheimer’s. Brain scans have shown that 17 to 22 percent of participants in Alzheimer’s studies in the recent past did not have amyloid plaque and may not have actually had the disease. And 36 percent of failed phase 3 drug trials from 2004 to 2021 didn’t test participants for the presence of amyloid plaques or tau tangles, meaning their cognitive problems could have been due to something else. “You’re never going to get a positive result when you’ve got the wrong people in the trial,” says Catherine Mummery, head of clinical trials at University College London’s Dementia Research Centre.
1906
the year German psychiatrist Alois Alzheimer discovered the brain disease
Another major issue: Researchers may have been too narrowly focused on one culprit. One-quarter of the failed drugs were aimed at amyloid plaques—globs of protein in the brain that were first spotted 118 years ago by German psychiatrist Alois Alzheimer in the brain of a woman with severe dementia. Since these sticky blobs were the defining feature of the disease, it made sense that they were the primary target of researchers.
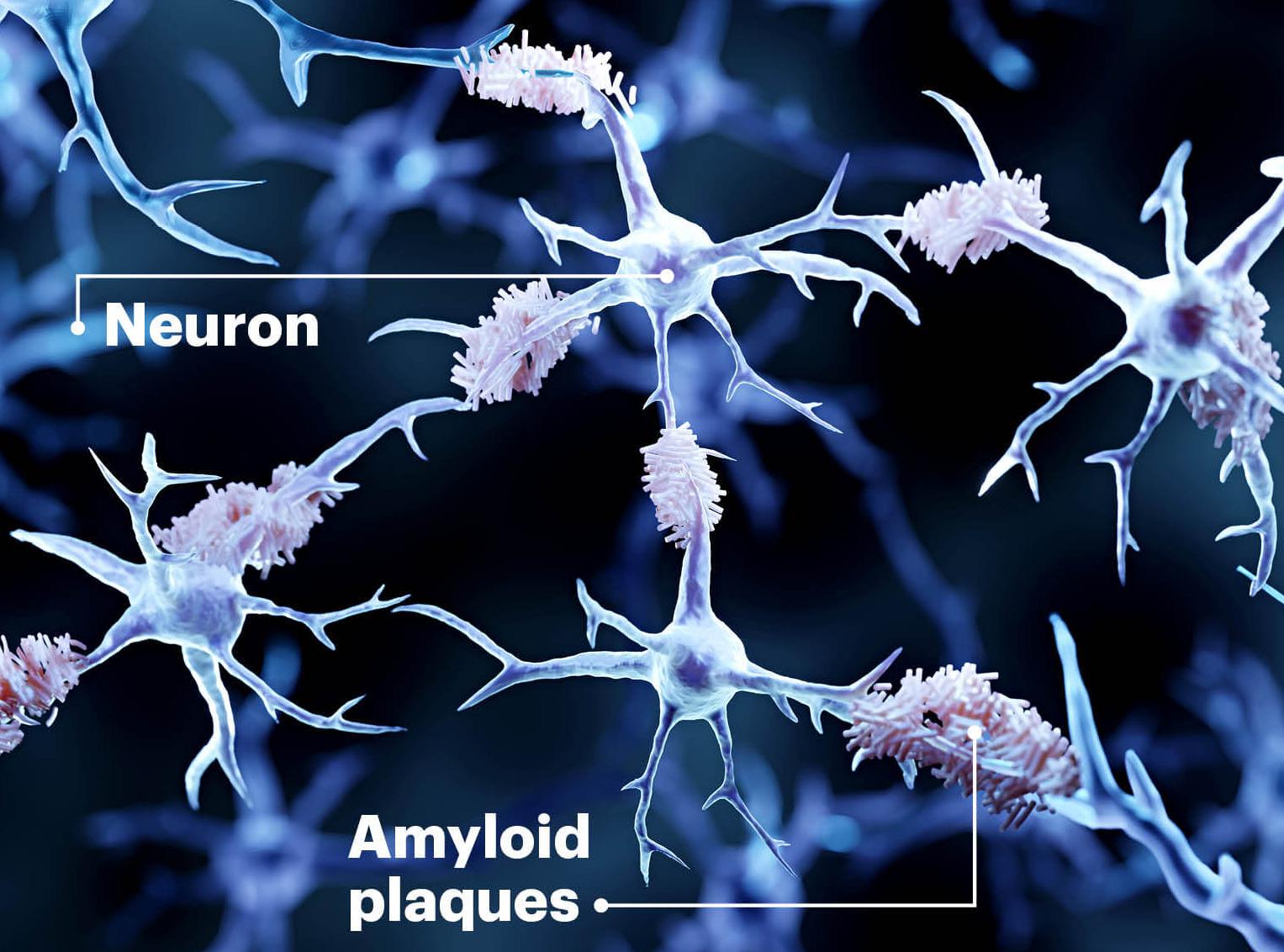
“The reason we’ve been so focused on plaques for so long is that they really stand out as soon as you look at the brains of people with Alzheimer’s disease,” says Kyle Travaglini, a scientist at the Allen Institute for Brain Science in Seattle, where he is part of a team creating an atlas cataloging how thousands of different types of brain cells are changed in Alzheimer’s disease. “You see these giant, ugly balls all over the brain. It wasn’t unreasonable to look at them initially.” Yet drug after drug developed to target the amyloid plaques—most notably aducanumab, an earlier drug similar to lecanemab that was recently discontinued—failed to show any clear impact on the cognitive decline of patients. Lecanemab is the first to show even modest success. Donanemab, which also clears amyloid plaques and slows disease progression, is expected to receive full FDA approval this year. And researchers are beginning to look at using focused ultrasound to open the blood-brain barrier and amp up the effectiveness of anti-amyloid drugs. In January, a West Virginia University study of three people that combined focused ultrasound with drug infusions removed more amyloid than the drug alone.
NEW APPROACHES, NEW HOPE
Other theories about what triggers Alzheimer’s are getting more attention—and drugs that target culprits other than amyloid are moving into early- and late-stage human trials. In 2016, 56 percent of disease-modifying Alzheimer’s drugs in human studies were aimed at amyloid plaque. By 2023, of 141 treatments in human trials, 84 percent were not for amyloid. Fillit says the intensity and variety of research—and lessons learned during years of frustration—should lead to faster progress.
Targeting amyloid is significant, he says, “but it’s not the whole story.” There’s a growing consensus that several factors might work together to cause the disease. Researchers continue to study amyloid plaques, but other human trials are underway on drugs designed to reduce brain inflammation, protect synapses (parts of brain cells that communicate with each other) and improve aspects of brain metabolism (such as processing blood sugar, the brain’s preferred fuel).
In particular, researchers are taking a harder look at tau tangles, globs of protein that form inside the brain cells themselves. One medicine attracting a lot of attention is called BIIB080. In a trial led by Mummery at the University College London, it was the first anti-tau drug to successfully remove these damaging protein tangles from brain cells in a human study.
BIIB080
an investigational anti-tau drug that successfully removed the toxic protein from brain cells
“Tau tangles in the brain seem to mirror much closer to the cognitive symptoms people have,” Bateman says. “A lot of us think that’s a clue. If we could neutralize tau, people’s symptoms could be better managed.”
At the University of California San Francisco (UCSF), a study called the Alzheimer’s Tau Platform recently won a $151 million grant from the National Institutes of Health (NIH) to test two anti-tau drugs plus an anti-amyloid drug that will be given together to 900 people with early-stage disease. “At a certain point with amyloid accumulation, tau gets sparked like a forest fire that really starts to do damage,” Mummery says.
On a different front, Finnish researchers launched a study that combines brain-healthy lifestyle steps with metformin, a diabetes drug that might improve blood sugar processing in the brain. The study will look at the effects of lifestyle plus the medication in people at risk for Alzheimer’s and dementia who do not have thinking and memory problems.
“The brain is only 3 percent of body weight but uses 20 to 25 percent of the body’s energy, mostly from glucose,” Fillit explains. Trouble absorbing blood sugar, called insulin resistance, increases with age. “If the brain is deprived of energy, neurons can die,” says Fillit, whose foundation helps fund the study. “We want to see if the combination would have more benefit than either one alone.”
Having drugs against these various factors, Fillit says, means that within 10 years, customized, multidrug treatments will likely be prescribed based on a simple blood test. (An analogy would be our approach to treating heart disease, which might involve cholesterol medications, blood pressure pills, blood sugar controls, dietary changes or a combination of these treatments.)
“We are starting to give combination drugs in trials,” Mummery says. “I believe that in 10 years’ time, we will have blood biomarkers that give a fingerprint of what your disease looks like. We’ll be able to use that to define an individualized treatment regime. We’ll be thinking about brain health in terms of prevention more than just dementia symptoms.
“I’m an optimist,” she adds. “We have a foundation. Once you have that foundation, research can accelerate.”

Linda Van Eldik in her lab at the University of Kentucky. She says chronic inflammation, by overwhelming the immune system, may be an underlying cause of Alzheimer’s.
IS YOUR BRAIN ON FIRE?
“I’ve always been intrigued by inflammation,” says Linda Van Eldik, director of the Sanders-Brown Center on Aging and the Alzheimer’s Disease Research Center at the University of Kentucky in Lexington. She says chronic inflammation may be one of the primary drivers of Alzheimer’s.
Van Eldik studies microglia, immune cells that patrol the brain by the tens of billions. Normally they work like trash trucks, gobbling up little scraps of amyloid protein waste before it can cause trouble. But when overwhelmed by inflammation, microglia pump out a torrent of inflammatory chemicals called cytokines. “Cytokines damage nerve cells [neurons] and synapses, reducing communication between cells,” she explains. It’s a vicious cycle. When cells are damaged by cytokines, microglia “start producing more inflammation, you get more damage, then you get more inflammation,” Van Eldik says.
Controlling neuroinflammation is at the forefront of new drug ideas for Alzheimer’s. In 2023, there were more drugs in human trials for inflammation than for any other target.
This may explain why aging, head injuries, stroke and other brain insults increase risk for Alzheimer’s and other dementias, she says.
Van Eldik’s NIH-funded research includes versions of an anti-inflammation drug candidate that blocks microglia from overproducing inflammatory compounds without stopping their normal trash-collection duties, she says. In phase 1 clinical studies, the drug was found to be safe in healthy adults. It is currently being tested in people who had strokes caused by brain bleeding and with brain cancers treated by radiation. If successful, Van Eldik expects the drug will be tested next in people with Alzheimer’s. She also expects it to be used in other cell-damaging brain conditions in which abnormal inflammation plays a role. “This drug has the potential to be a first-in-class disease-modifying therapy for Alzheimer’s disease and related dementias,” Van Eldik says.
Controlling neuroinflammation is at the forefront of new treatment ideas for Alzheimer’s, Fillit agrees. In 2023, there were more drugs in human trials for inflammation than for any other Alzheimer’s disease–modifying factor, and Fillit says inflammation drugs could be among the first Alzheimer’s compounds to win FDA approval in the next three to five years.
THE BATTLE ON THE HOME FRONT
The difficulty in diagnosing Alzheimer’s accurately has long hindered scientists’ ability to study the disease. Historically, it could be confirmed only by examining the brain after death. Today, researchers can make a firm diagnosis of Alzheimer’s by spotting amyloid plaque via positron emission tomography (PET), or by testing for its presence with a lumbar puncture, says Ronald Petersen, M.D., a Mayo Clinic neurologist and Alzheimer’s researcher. “But the first one is expensive. And the second one is invasive.” So they’re not routinely used.
New and on-the-horizon blood tests that measure amyloid and tau in the brain aid researchers in tracking brain changes during studies. These blood tests are beginning to be used in doctors’ offices. Sperling expects tests to be available in the next year showing not just how much amyloid is in the brain but whether it is triggering the explosion of tau that seems to torpedo thinking and memory. This could help, in the future, determine risk in people who do not have Alzheimer’s symptoms. “We’re going to do a much better job of predicting individual risk,” she says.
That’s significant not just for treatment but in terms of prevention as well. For all the deep science that surrounds the war on Alzheimer’s, one of the most important weapons against the disease remains the simplest: healthy living. In that way, late-life Alzheimer’s resembles heart disease, diabetes and many other chronic conditions linked to aging: There is a genetic component, yet so much of prevention is in our own hands. A 2022 University of Minnesota study found that an estimated 41 percent of Alzheimer’s and related dementias were attributed to a dozen modifiable risk factors, of which high blood pressure, obesity and physical inactivity had the most impact.
“People need to know, ‘What are my risk factors for Alzheimer ’s and other dementias, and are they things I can do something about?’” says Kristine Yaffe, M.D., director of the Center for Population Brain Health at UCSF. Yaffe was the lead researcher on a November 2023 study of 172 adults ages 70 to 89 who had two or more risk factors for dementia. Those who worked on one or more personally chosen risk factors for two years boosted their scores on tests of thinking and memory and lowered their dementia risk more than those who simply received educational materials.
41%
of Alzheimer’s and related dementias were attributed to a dozen modifiable risk factors, including high blood pressure, obesity and physical inactivity.
“Instead of a one-size-fits-all program, we wanted to see what would happen if we personalized it,” Yaffe says. Strategies included taking care of high blood pressure, diabetes and/or depression; exercising; getting sound sleep; socializing; and quitting smoking.
Dean Ornish, M.D., founder of the nonprofit Preventive Medicine Research Institute and clinical professor of medicine at UCSF, is directing the first randomized controlled trial to determine if the same lifestyle changes that he pioneered to reverse coronary heart disease might slow, stop or reverse the progression of mild cognitive impairment due to Alzheimer’s disease. “What’s good for your heart is also good for your brain, because they share many of the same underlying biological mechanisms,” Ornish says. “We’re at a state of evidence with Alzheimer’s similar to where we were 45 years ago with coronary artery disease. At that time, it was thought that heart disease could only get worse. We found that bigger lifestyle changes could often reverse the progression of heart disease. We are studying if the same may be be true for mild cognitive impairment due to Alzheimer’s disease as well. One man shared, ‘I have a sense of hope.’” UnDo It!, a book Ornish wrote with his wife, Anne, describes his lifestyle medicine program for both heart disease and Alzheimer’s.
Prevention studies using drugs are gearing up. Researchers study medications like lecanemab in people with early evidence of Alzheimer’s brain changes who do not yet have life-changing thinking and memory problems. In the future, Sperling says, drugs could be started before memory troubles appear—the way people with high cholesterol take statins to lower risk for a heart attack and those with diabetes take blood-sugar-lowering drugs to protect against complications such as kidney disease.
“This is the way forward,” she says. “It’s exactly what we do in heart disease and diabetes. We lower cholesterol before someone has a heart attack. This is what we have to do in Alzheimer’s disease.
“For the first time, it’s very feasible.”
Sari Harrar is a contributing editor for AARP The Magazine and frequently writes on health for the Bulletin, including recent cover stories on cancer and heart disease.