Cover Story

COVID:
Where We Are Now —
Where We’re Headed
COVID-19 isn’t slowing down. In at least 42 states, COVID cases, emergency room visits and hospitalizations all spiked this summer. In June, more than 1 in 50 Americans 65 and older went to an ER and were diagnosed with COVID, more than double last summer’s rate, a rise attributable to the highly contagious omicron strains known as FLiRT.
FLiRT strains account for the majority of new cases, according to the Centers for Disease Control and Prevention.
Summer spikes happen when people huddle inside in air-conditioning for Father’s Day, graduations and similar events. But older Americans should be concerned about what lies ahead. For the past two years, COVID infections among people 65 and older were highest between Thanksgiving and Valentine’s Day, peaking around Christmas each year. “It is likely we will see more cases as we move into fall/winter,” says Pragna Patel, M.D., senior adviser for long COVID at the CDC. For the past two winters, more than 1 in every 20 Americans 65 and older wound up in an ER with COVID symptoms.
FLiRT variants spread easily, having mutated to evade some antibodies. They don’t appear to cause more serious symptoms—doctors see everything from mild colds to severe respiratory infections. It’s not that they’re any less deadly, but most of us have acquired a certain degree of immunity to COVID-19.
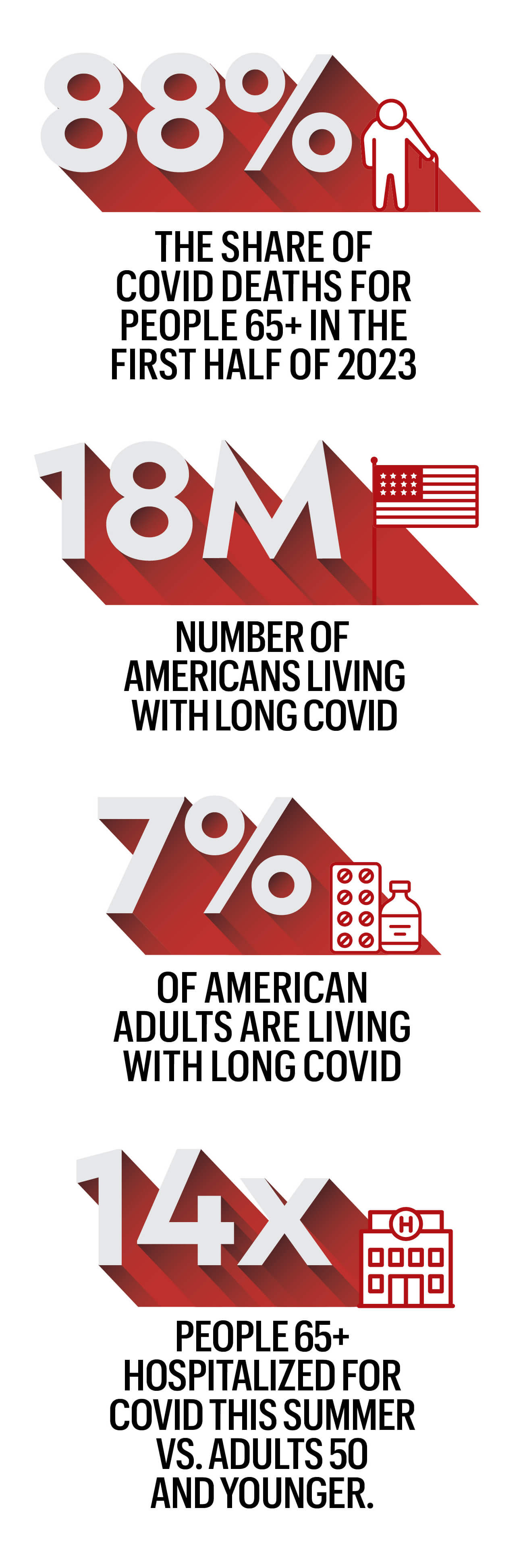
Still, older adults remain at risk. Early this summer, hospitalization rates for those 65 and older were roughly 14 times higher than for adults under 50, according to the CDC. For older Americans, then, protecting ourselves is critical. Here’s how.
▶︎ Get your vaccinations up to date—pronto. Vaccination is still paramount for preventing COVID and decreasing the risk of severe illness and death, says Sara F. Martin, M.D., medical director of the Adult Post-Acute COVID Clinic at Vanderbilt University. If you’re due for your next shot, there’s no reason to wait: Updated 2024–2025 COVID vaccinations from Moderna, Novavax and Pfizer are expected to roll out this month. Medicare Part B continues to cover the vaccine, as do most insurers, but it’s best to check in advance. Some insurers only cover the vaccine when it’s administered in network. And yes, it’s safe to get your flu shot at the same time.
▶︎ Don’t rely on prior immunity. “Protection wanes over time,” says William Schaffner, M.D., professor of preventive medicine and infectious diseases at Vanderbilt University School of Medicine. Because the older vaccines weren’t targeted to all of the FLiRT strains, you need this fall’s newest version.
▶︎ And don’t rely on a history of luck. Though there are folks out there known as novids—people who’ve never had COVID—that doesn’t mean you’re immune if you’re a member of that group. In fact, not having built-up antibodies to an actual infection could render you more likely to catch the disease, especially if you cruise on your previous luck and skip the vaccine updates.
▶︎ Protect yourself in high-risk areas. “The front line of prevention is still handwashing and masks,” says Jill Foster, M.D., assistant dean at the University of Minnesota Medical School. Be a religious hand washer and wear a mask if you’re at high risk or in a crowd.
▶︎ Have a Paxlovid plan. Antivirals such as Paxlovid help reduce the severity of illness and may help protect against the risk of long COVID. Starting treatment as soon as possible after testing positive for COVID is paramount. If you’re at high risk, it might make sense to talk with your doctor now about getting a plan in place in case you get sick, Schaffner says. “What would happen on a weekend, for example, or if your provider is on vacation? Just have that conversation so that, should you turn positive, [you’ll be able] to start your Paxlovid just as quickly as you can.”
▶︎ Stock up on home tests. Check your stash of home tests to make sure they’re not expired. Pick some up at your local pharmacy if you need up-to-date tests.
▶︎ If you test positive, you should remain isolated until you’ve been symptom-free for at least 24 hours without the use of fever-reducing medications, according to the CDC. Once symptoms pass, it’s still recommended that you take additional steps to prevent the spread of the disease for at least the next five days: Practice social distancing, wear a mask around others, ventilate your home if possible and wash your hands—especially if you’re around other older adults.
THE UNTOLD IMPACT OF LONG COVID
Even mild cases of COVID-19 are linked to potential long-term repercussions—some of them deadly serious. Here’s what we know about the aftermath of the disease

Chrissy Bernal with the supplements she needs to cope with food allergies caused by long COVID
Chrissy Bernal has caught COVID-19 three times, most recently in October 2023. “My symptoms were always pretty mild,” she says. But after her third round of the virus, she developed extreme allergies to foods she used to eat all the time: oats, dairy, gluten, sesame seeds and peanuts. “I literally have some level of anaphylaxis every single day,” she says. In May, Bernal, 46, a public relations professional in Houston, went into anaphylactic shock during a virtual meeting. “I had to inject myself with an Epi while everyone watched in horror on Zoom,” she says.
Natalie Nichols, 53, has been struggling with debilitating asthma and severe food allergies since she first caught COVID more than three years ago. “Last fall, I spent two-and-a-half months confined to bed, motionless, because moving, including holding a cellphone, made me too short of breath,” she says. She’s also experienced brain fog, high blood pressure, hyperglycemia, fatigue and gastrointestinal symptoms. Nichols, the founder of a nonprofit in Nacogdoches, Texas, recently underwent surgery to repair joint damage caused by COVID-induced inflammation.
Lorraine W., of Clarence Center, New York, was looking forward to an active retirement when she was diagnosed with COVID in March 2020. “I’ve never returned to my pre-COVID self,” says Lorraine, 65. She’s on medication to treat small blood vessel damage to her heart and continues to battle a lingering cough, fatigue and breathlessness, as well as kidney disease. Neurological changes have made her legs unsteady when she walks, requiring her to use balance poles. “None of these conditions were present before COVID,” Lorraine says.
In June, the National Academies of Sciences, Engineering, and Medicine released a comprehensive definition of long COVID: “an infection-associated chronic condition that occurs after COVID-19 infection and is present for at least three months as a continuous, relapsing and remitting, or progressive disease state that affects one or more organ systems.” According to that definition, 18 million Americans have experienced long COVID; currently, more than 1 in 20 of us are living with its symptoms. Researchers have begun to link long-term COVID with another recent phenomenon: our shrinking life expectancy.
THE DISEASE WE’RE FORGETTING
COVID doesn’t seem that scary anymore. More than 98 percent of the U.S. population has some degree of immunity—from vaccination, prior infection or both—and Paxlovid and other medications are available to counteract acute symptoms. For many of us, contracting COVID is like having a bad upper respiratory infection.
But “COVID isn’t gone,” says Ryan Hurt, M.D., director of the Long COVID Research and Clinical Program at the Mayo Clinic. The World Health Organization estimates that COVID still kills at least 1,000 people every week around the globe—but “we only have data from about 40 countries,” says Maria Van Kerkhove, M.D., director of WHO’s Department of Epidemic and Pandemic Preparedness and Prevention.
Older adults and those with preexisting conditions remain among the most at-risk populations for severe, acute COVID. People 65 and older accounted for 63 percent of COVID-related hospitalizations and 88 percent of in-hospital deaths during the first seven months of 2023, according to CDC data.
Although the dangers of acute COVID infection may have ebbed for many, the reality of long COVID is coming into view. Of those who contracted COVID-19 within the past four years, 10 to 20 percent have experienced long COVID.
“With every new case of acute COVID [the initial phase of infection when diagnosed or symptoms first appear], there is risk for developing long COVID,” says Caitlin McAuley, D.O., a family physician at the Keck COVID Recovery Clinic in Los Angeles. She’s had patients who developed long COVID fully recover, get reinfected several times with no lingering effects, then develop another case that leads to a new bout of long COVID. She also has seen patients who got COVID twice with no lingering effects, and the third time they ended up with prolonged symptoms.
“We still have a number of individuals who had the first wave of COVID who are suffering from long COVID symptoms now, several of them many years out,” says Jerrold Kaplan, M.D., medical director of the COVID Rehabilitation and Recovery Program at Gaylord Specialty Healthcare in New York.
Having escaped long COVID previously doesn’t mean you won’t face it in the future. Indeed, some research has suggested that catching multiple COVID-19 strains puts you at increased risk. A study published in 2022 found that reinfection can increase the risk of complications in major organ systems, and these risks persist at least six months beyond the initial infection.
We don’t yet know the true impact of catching COVID. “Many chronic disease processes, such as cardiovascular disease, dementia and cancer, take years to develop. And whether acute COVID-19 puts people at risk for some of these issues? Time will tell,” Hurt says.
What doctors do know is that patients are flocking to their offices complaining of symptoms they never had before COVID.
IS LONG COVID BOOSTING OUR DEATH RATE?
In July, COVID accounted for less than 1 percent of all deaths in the U.S. Life expectancy in the U.S. is 77.5 years, reflecting an uptick over the past two years but still lower than prepandemic levels. Many factors contribute to that statistic, but it’s clear that the long-term effects of COVID have played a role.
For example, a study in the journal Nature Medicine found that those hospitalized with COVID had a 29 percent greater risk of death in the three years after their infection.
“But what was also alarming is that in people who weren’t hospitalized, there was also an increased risk of a variety of medical issues,” says John Baratta, founder and codirector of the COVID Recovery Clinic at the University of North Carolina at Chapel Hill. Even patients who’d had mild bouts of COVID-19 had an increased risk of respiratory, cardiovascular, metabolic and neurological issues lingering for three years after the initial infection. Long COVID patients had a significantly increased risk of severe health issues affecting the brain, lungs and heart.
We have long known that an acute case of COVID can compromise heart health: Compared with those who didn’t contract COVID, people who caught the virus were 81 percent more likely to die of a cardiovascular complication in the ensuing three weeks, according to a study of 160,000 patients published by the European Society of Cardiology. But the risk lingers long after the symptoms abate. Those who caught the virus were five times more likely to die from cardiovascular disease as long as 18 months after infection, the same study found. Heart disease deaths, which had been on a downward trend for decades, began to spike in 2020 and remained high through 2022, the last year for which data is available.
Stroke, blood clots in the legs leading to clots in the lungs, abnormal heart rhythm (arrhythmia) and inflammation of the heart are among the challenges COVID poses, says Mohanakrishnan Sathyamoorthy, M.D., professor and chair of internal medicine at the Burnett School of Medicine in Fort Worth, Texas. In long COVID, this collection of cardiovascular disruptions can present as postural orthostatic tachycardia syndrome (POTS), in which patients’ heart rates increase abnormally when they go from sitting or lying down to standing up.
One theory to explain COVID’s long-term effect on the heart—and the body in general—centers on inflammation. “Every time you get infected with COVID, there is a possible increased risk of long COVID, and some cardiac disorders can occur—especially if you have a history of heart disease, including stroke, heart disease and heart attacks,” says Pragna Patel, M.D., senior adviser for long COVID at the CDC. All of these problems can be exacerbated by the virus entering coronary tissue and triggering inflammatory responses that can damage the heart.
Researchers say COVID may also alter the gut microbiome, a primary controller of inflammation, thereby triggering the immune system to rev up the condition. “There is no single agreed-upon mechanism that’s causing the issues,” Baratta says. “An individual may have multiple factors going on in their body, and not everyone will have the same underlying mechanism causing their symptoms,” which increases the complexity of both research and treatment.
One factor that seems to matter: vaccination status. “Several studies show that vaccination can decrease the risk of developing long COVID,” Patel says. Vaccination rates tend to increase with age, with people 75 and older being the most well vaccinated—hence the most well protected from long COVID, Patel theorizes. That may explain why long COVID most commonly affects people ages 35 to 64; the risk seems to drop for those 65-plus, according to CDC data.
FROM LONG COVID DIAGNOSIS TO TREATMENT
No single test can determine whether a person has long COVID. Doctors typically diagnose long COVID by reviewing the patient’s health history and current symptoms and trying to rule out other causes. A positive COVID test is not required, as someone could have been infected without knowing it, then experience strange symptoms later, Patel says.
Though there are many ongoing clinical trials on long COVID, there is no umbrella treatment. Primary care physicians address what they can, then call in specialists—such as a cardiologist to handle arrhythmia or a therapist to treat anxiety—for more targeted care. There are long COVID centers around the country where teams of professionals work to help patients through their unique symptoms. “Because the effects of COVID are so wide throughout the body and mind, there will not be a single treatment for all long COVID issues,” Baratta says. “This is going to be treated by many different types of providers and specialists, and it will be treated, often, symptom by symptom.”
Long COVID is recognized as a disability under the Americans with Disabilities Act if it substantially limits one or more major life activities. About 200 symptoms fall under that umbrella, Patel says. Here are some of the conditions we’re learning can linger months and, in some cases, years beyond an acute COVID infection. If these or other health changes seem familiar, consult your primary care physician.
1. EXTREME FATIGUE
It’s common to experience fatigue when your body is busy fighting off an illness. But some people still struggle with fatigue long after their initial COVID infection. In fact, a lack of energy is the number one symptom reported by long COVID patients. In some, this can be diagnosed as chronic fatigue syndrome, which has been on the rise since the start of the pandemic, Baratta says. He defines this as “a disabling level of fatigue that severely limits daily activities.”
This lingering fatigue may be due to limited production of energy within the muscles caused by damage to the mitochondria from a COVID infection. It can happen to anyone—no matter their level of fitness before infection. “I’ve treated patients who have been triathletes and now may only be able to do 15 or 20 minutes of exercise a day, when they’re used to running and swimming miles at a time,” Kaplan says. He recommends starting slow and pacing yourself with everything you do around the house, “doing shorter intervals several times throughout the day, rather than trying to do everything at once.” Whether it gets better depends on the individual. Some people’s symptoms clear, and some people may battle them indefinitely.
2. SHORTNESS OF BREATH
An analysis of chest CT scans from 144 patients ages 27 to 80 found that more than one-third of people hospitalized with a previous COVID infection had lung scarring and thickening two years after coming into contact with the virus. Even patients with milder cases who walked away without scarring can experience changes in their breathing.
“Some research shows that people after COVID start to take shorter, shallower breaths,” Baratta says. “This essentially causes a type of hyperventilation they are doing without even recognizing it, not getting good fresh air deep into the lungs, and [this] can lead to shortness of breath.” Doctors have found success using respiratory exercises to help patients relearn slow, deep breathing.

3. COGNITIVE CHANGES
Difficulty concentrating, spaciness and forgetfulness are just a few of the brain challenges COVID can bring on. These can last for weeks or months or—in some with long COVID—become an everyday occurrence that lasts indefinitely. COVID may linger in a person’s gut long after an infection, altering their microbiome and hindering the body’s ability to produce serotonin, leading to cognitive disturbances.
COVID may also disrupt the blood-brain barrier, allowing chemicals or molecules in the rest of the body to enter the brain blood circulation and potentially lead to brain fog, Baratta says.
One study found that 30 days after testing positive for COVID-19, people were at greater risk for cognitive decline, as well as for mental health disorders including anxiety, depression and stress. Another study found inflammation in the brains of people with mild to moderate COVID-19 was similar to the effects of seven years of aging. Doctors are leading neurologically affected patients through cognitive rehabilitation exercises that show promise in reducing symptoms.

4. DEPRESSION AND ANXIETY
“Mood-related disorders are one of the top five issues that happen to people after COVID,” Baratta says. There may be a direct relationship between the virus’s effect on the brain and mood issues. A 2021 review of eight studies found that 12 weeks after a COVID infection, 11 to 28 percent of people had depression symptoms, and 3 to 12 percent of those individuals reported their symptoms as severe. If you’re feeling more stressed or down after catching COVID, tell your primary care physician, who can refer you to a therapist. Or visit the American Psychological Association’s search tool at locator.apa.org to find a qualified therapist in your area.

5. SLEEP DISTURBANCES
Nearly 40 percent of people with long COVID have reported major changes to their sleep patterns. One study looked at 1,056 COVID-19 patients who did not have a severe enough infection to require hospitalization. Of that population, 76.1 percent reported having insomnia and 22.8 percent severe insomnia. Sleep apnea may also appear post-COVID, another way the disease affects the respiratory system.
Talk to your doctor if you’re having sleep issues. A CPAP (continuous positive airway pressure) machine can help with sleep apnea. Lifestyle habits that prioritize healthy sleep, such as keeping consistent sleep and wake times and avoiding large meals before bed, may also help. “Post-COVID sleep has literally been a nightmare! We saw a 23 percent increase in sleeping-pill prescription during and post-COVID,” says Michael Breus, a clinical psychologist and clinical sleep specialist in Los Angeles.

6. DIGESTIVE UPSET
Diarrhea, constipation, abdominal pain, bloating and gas: These symptoms of irritable bowel syndrome can be by-products of an encounter with COVID. A survey of 729 COVID survivors found that 29 percent experienced at least one new chronic GI symptom six months after their infection. “There is evidence that parts of the COVID virus linger in the GI tract for many months after the initial illness, and it’s been suggested that the presence of these ongoing viral fragments causes dysfunction or problems with the GI tract, leading to mostly symptoms of diarrhea and gastric distress and discomfort,” Baratta says.
Talk to your doctor about any new digestive symptoms or seek help from a gastroenterologist. You can keep a food journal and note if your condition flares after eating certain foods. Try cutting out those foods, then reintroducing them one by one to see what you react to, Kaplan advises.
7. NEW OR WORSENED ALLERGIES
Some people who develop COVID experience allergies they never had before. One study found the risk of developing allergic diseases, such as asthma and allergic rhinitis, rose significantly within the first 30 days after a COVID diagnosis. This may be because one’s immune system stays hypervigilant after fighting the virus, McAuley says.
In severe cases, like Chrissy Bernal’s, this can lead to mast cell activation syndrome (MCAS), a disease that can behave like a series of severe allergies: The body’s cells become hypersensitive, causing strong reactions to everything from food and pollen to even a hot shower or exercise. Antihistamines and other medications may help, so talk to your doctor if you experience skin itching, a rapid pulse, wheezing or gastrointestinal symptoms.

8. PAIN
Some COVID survivors battle chronic pain, everything from aching joints to testicular pain. There is a higher risk of inflammatory arthritis, and women are at higher risk than men. One review of studies estimated that 10 percent of people who contracted COVID experienced musculoskeletal pain at some point during the first year after infection.
Reducing stress, eating a healthy diet and exercising may ease some post-COVID discomfort. Massage therapy, movement therapy, acupuncture and over-the-counter pain medications may also offer relief. Your doctor can refer you to a specialist, such as a rheumatologist, who can help manage symptoms including joint pain.
FAST-MOVING RESEARCH MEANS NEW HOPE
If your symptoms last after a bout of COVID, start with your primary care physician, who can help treat your symptoms or refer you to a specialist. Despite previous dismissals, long COVID is more recognized these days, Patel says, and the CDC is doing its part to educate both patients and providers. And initiatives such as the National Institutes of Health’s Recover program are researching treatment options.
“In a year, things will look different, because research is moving so quickly,” says Sara F. Martin, M.D., medical director of the Adult Post-Acute COVID Clinic at Vanderbilt University Medical Center. The CDC, for instance, is funding a series of clinical trials that the NIH has in the works. This new information, Martin says, may guide doctors, including herself, who treat long COVID patients to better ease their symptoms.
Nicole Pajer writes regularly for Self, Glamour, Parade and other national magazines.
HOSPITALIZATION RATES ASSOCIATED WITH COVID-19
